
The Centers for Disease Control & Hypocrisy?
Last week, the Centers for Disease Control and Prevention released a highly contentuous new Vital Signs post on women, pregnancy, and alcohol. The main message was, essentially “don’t drink, ever, if you could possibly be using your uterus to store more than endometrial tissue, fibroids, or intrauterine devices.” 
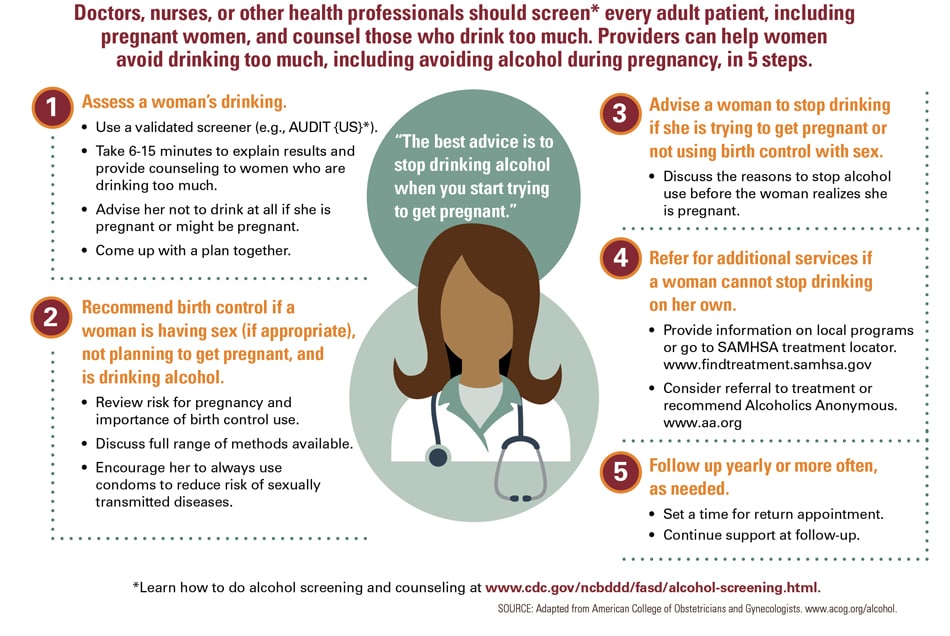
Now, while studies don’t support the idea that mild drinking while pregnant will harm a fetus, the CDC (and many commentators) have latched onto this rather ludicrous THE RISK IS REAL DON’T TAKE ANY RISK approach for alcohol and pregnany, even going so far as to say it’s not worth risking a single IQ point.1 Let’s say we accept this fearmongering approach, ignoring the lack of scientific support for the assertions, ignoring the victim-blaming nature of the infographic,2 even ignoring the fact that the CDC conveniently forgot not only a man’s role in conception but the damage drinking can do to sperm and how that can affect fetal development.3 Any risk is bad. Wrap pregnant women up in cotton, leave them in a padded room, and don’t let them do anything in case they happen to be in the process of 9.5-odd months of gestation.
Really don’t let them smoke, right? I mean, the risk is real! Smoking while pregnant can cause fetal death, low birth weight, preterm birth, affect the integrity and function of the placenta, is a risk factor for sudden infant death syndrome—oh my gosh! This list is just as bad, if not worse, than the risks of pregnancy and drinking for fetal alcohol spectrum disorders. Certainly with the release of new data on the risks of smoking and pregnancy—completely separate from the other known risks that smoking has on health, such as cancer, emphysema, chronic obstructive pulmonary disease, and death—the CDC has created an equally dire infographic and message saying that the risk is real, so quit smoking, why take the risk?
Yeah, nope.
We didn’t even get an infographic.
Instead, we got a very sensible, calm, factual question-and-answer style statement from the CDC explaining how smoking can harm a pregnancy and baby, the number of women who smoke while pregnant, benefits of quitting, effects of second-hand smoke, and further resouces, with various facts hyperlinked within the article itself.
It’s almost an ideal example of how to present facts about a risk in order to allow women to do an analysis of the situation based on their own agency and autonomy.
The CDC did everything right this week with their publicization of new information about smoking and pregnancy data and risks. As Sarah Richardson and Rene Almeling noted in the Boston Globe on Monday, “[w]omen are constantly bombarded with advice about what to eat and drink and how to behave during pregnancy,” and rather than add to the growing list of simplistic injunctions of an “omg if you do that you will kill the baby” variety, the CDC provided pregnant people with credible information about how to weigh reproductive risks.
And yet. And yet. In the light of last week’s NO RISK IS ACCEPTABLE message regarding women and pregnancy, it’s a stark difference in approach and messaging, and both underscores the hypocrisy of their “ABSTAIN OR ELSE” message regarding alcohol while further damaging their credibility as a trusted source of health information and regulation.
 First, the CDC needs to be clear that science on the risk of alcohol during pregnancy is far from settled. Any advice about reproduction should respect the autonomy and intelligence of women by presenting evidence in its full context. Public health officials should provide perspective about the size of the effects relative to other common risk factors. And they should be straightforward in describing the evidentiary base for health advisories.
First, the CDC needs to be clear that science on the risk of alcohol during pregnancy is far from settled. Any advice about reproduction should respect the autonomy and intelligence of women by presenting evidence in its full context. Public health officials should provide perspective about the size of the effects relative to other common risk factors. And they should be straightforward in describing the evidentiary base for health advisories. On the surface, the One Key Question Initiative, by the Oregon Foundation for Reproductive Health, may seem like a good idea. Many women have access to a primary care provider, but do not see OB-GYNs with any regularity. And of course, discussing reproductive and contraception options with a patient should be a basic of yearly, preventive, or wellness exams. The problem is not in discussing reproductive and contraception options, but instead in the framing of the question: would you like to become pregnant in the next year?
On the surface, the One Key Question Initiative, by the Oregon Foundation for Reproductive Health, may seem like a good idea. Many women have access to a primary care provider, but do not see OB-GYNs with any regularity. And of course, discussing reproductive and contraception options with a patient should be a basic of yearly, preventive, or wellness exams. The problem is not in discussing reproductive and contraception options, but instead in the framing of the question: would you like to become pregnant in the next year?
 One thing still sticks in my craw: the utterly ludicrous suggestion from respected epidemiologist Michael T. Osterholm that we were all just afraid to talk about
One thing still sticks in my craw: the utterly ludicrous suggestion from respected epidemiologist Michael T. Osterholm that we were all just afraid to talk about 
